What Is MUST?

Pictured above: Marsden M-600 Hoist Weighing Attachment.
You may have seen us mention MUST a few times in our previous blog posts, such as this blog about accurate weight assessments in care homes. But you may be asking yourself, what is MUST?
MUST, or the Malnutrition Universal Screening Tool, is a five-step screening tool that is used to identify whether adults are malnourished, at risk of becoming malnutrition or obese.
What Is MUST?
MUST was developed in 2003 by the British Association for Parenteral and Enteral Nutrition (BAPEN) and is widely used across more than 80% of hospitals and care homes in England and 98% in Scotland. It has even been taken up in some nordic countries.
Nursing staff carry out MUST both on admission and regularly during a patient’s stay to look out for any weight loss.
How Does MUST Work - The 5 Simple Steps:
1. Measure the Height and Weight of a Patient to Get a BMI Score
The first step of the MUST framework is to get an accurate height and weight for a patient. A reliable scale with a height measure should be used to do this to ensure that a precise BMI is also recorded.
We’d recommend using the Marsden M-100 Column Scale with Height Measure for this step. However if the patient is immobile and is unable to stand on the floor scale then we recommend the Patient Transfer Scale as a comfortable alternative. Hoist Scales, Bed Scales and Chair Scales may also be suitable in this scenario.
Some of these scales may come with a BMI function, which simplifies this step. Simply press the BMI button on the scale, enter the patient's height, and it will automatically calculate their BMI.
Alternatively, use the chart below to calculate a patient's BMI using their weight and height.
The BMI then results in a score out of 2.
>20 (>30 obese) = 0 | 18.5 - 20 = 1 | <18.5 = 2
2. Note the Percentage of Unplanned Weight Loss and Score
Again this is calculated using a table, although it’s hard to get an accurate result when patients are first admitted as they may not be aware of their previous weight.
For estimating whether new admission patients have recently lost weight, look at their clothing or jewellery. Is it loose fitting? This can be a key indicator.
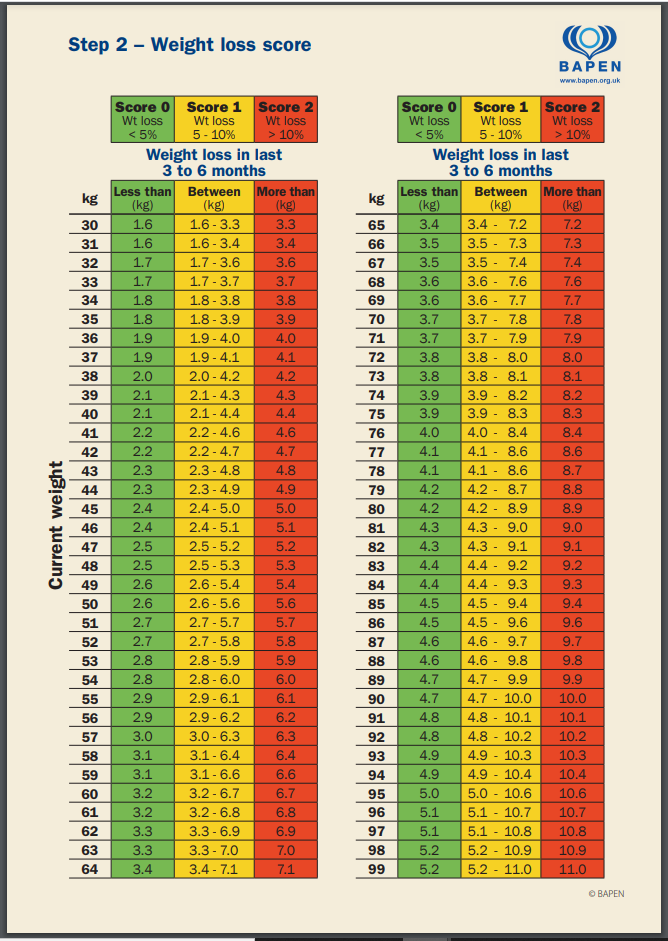
Look up the current weight of the patient in the left hand column and, using their previous weight, calculate how much weight has been lost in the past 3 to 6 months. Once again, this is then scored out of 2, with a weight loss of more than 10% resulting in a score of 2. A weight loss of between 5-10% scores a 1 and less than 5% results in a score of 0.
3. Establish Acute Disease Effect and Score
If the patient is ill and it’s significantly affecting food consumption, resulting in (or is likely to result in) little or no nutritional intake for more than 5 days, then take a score of 2.
4. Calculate the Final Score
Using the scores from the previous steps, calculate a patient’s overall risk of malnutrition.
If a patient receives a score of 0, then they are at a low risk. A patient with a score of 1 is a medium risk and any patient with a score of 2 or higher is considered high risk.
5. Use the Management Guidelines to Decide on the Next Steps
Using the scores from the previous steps, calculate a patient’s overall risk of malnutrition.
If a patient receives a score of 0, then they are at a low risk. A patient with a score of 1 is a medium risk and any patient with a score of 2 or higher is considered high risk.
Depending on the level of risk you have assigned to a patient, this next step will vary.
If a patient has been established as a low risk, then no further action is required. Simply continue routinely weighing the patient to screen for any malnutrition issues that may develop later. Hospital patients should be checked weekly, while it's recommended that care home patients are checked every month and community patients are checked every year.
Medium risk patients require observation. Their nutritional intake should be monitored and recorded for 3 days and if it’s adequate then routine screening should be resumed. This should be carried out more often, however, especially community patients, who are recommended to be checked every 2-3 months, instead of annually.
For clinical concerns when it comes to their dietary intake, then it's important to follow local policy and set goals to improve and increase over intake. The care plan should be monitored and reviewed regularly.
When a patient has been classified as high risk, then immediate action must be taken. The patient should be referred to a dietician or a nutritional support team. As with the previous risk level, goals should be set to improve and increase nutritional intake and this care plan should be reviewed weekly in hospitals and monthly in care homes or community settings.
Related Products
Further reading
Monitoring the weight of residents is very important. Find out why accurate, regular weight assessments are needed in care homes in this blog post.
MUST can also be used to screen for obesity. In this blog post, we look at the five unexpected causes for rapid weight gain.
The risk of being undernourished increases significantly with age. That’s why it’s important to monitor weight loss in older patients.